Dear Caregivers, Do you ever have questions if you are puréeing your food correctly for your loved one on a puréed diet? The number one question I get on initial visits is what can I feed them, followed by what is puréed food supposed to look like, and lastly how do I do it?
Having to prepare foods for a person on a puréed diet can provoke lots of worries, anxieties and fears about doing it right. Understandably, carrying the burden of responsibility to provide another persons daily nutrition and hydration needs on top of the need for a specialized diet consistency for their health is enough to increase the stress levels of a caregiver exponentially.
In this post, I will explain the definition of puréed food that is used by institutions worldwide. Does your puréed food have to look the same as what the food looked like when your loved one was in the hospital or rehabilitation setting? I will answer this question of what this means for a caregiver in the home setting.
I’ve seen over the years many terms and labels used to describe the various diet consistencies a person can be put on according to their specific swallowing problem. These diet consistencies are designed to make a person with swallowing problems safer by eliminating or decreasing their risk of choking, aspirating and /or causing or exacerbating respiratory illnesses.
A modified diet may also be used for maximizing oral intake by making the consistency easier to swallow, or for conserving a person’s energy when eating or drinking, or a temporary measure for a person to recover from a severe illness, surgery, injury or delirium.
Introduction & History of IDDSI:
In 2013, a group of experts in the field of dysphagia joined forces to develop a universal standard for managing dysphagia through diet modifications. The goal was to create standardization that would clarify terminology and guidelines among healthcare providers, caregivers and patients to improve consistent care and improve safety risks for individuals with dysphagia.
This global collaboration group of professions designed a framework that was named International Dysphagia Diet Standardization Initiative. Over the next couple of years they did research and released the first framework in 2015 that introduced a continuum of levels for drinks and foods.
In 2016 adjustments were made and a final framework for IDDSI was published. The framework provided detailed descriptions and testing methods to determine the appropriate level of food and drink texture.
2017-2019 was focused on promoting the adoption of the framework worldwide. The creation of educational material, training programs and resources were made available to facilitate implementation in various healthcare settings.
The adoption and implementation of IDDSI has made a powerful impact on improving the management of dysphagia globally. It has been supported by major organizations. The initiative continues to promote education, collaboration and research to offer a consistent and evidence-based approach to diet modification.
TIP: There are other diet consistency terms still being used to describe various modified textured levels . You may see terms such as mechanically altered, dysphagia diet, mechanical soft or dysphagia advanced. I ask the dietary department personnel what terms they use and how the food is prepared for each level they provide at any particular setting.
Puréed Food Guidelines & Tests Per IDDSI:
The IDDSI official website, IDDSI.org has PDF files that can be printed with their licensing laws and regulations for use of their materials. Their website has easy to read material . It has detailed descriptions, pictures and information on how to test for each level consistency for foods and liquids.
There are guidelines for Level 0 – Level 4 for liquids and Level 4 – Level 7 for foods. The following information has come from their online material. For the purpose of this post, we are focusing on puréed foods.
Level 4 – Pureed food.
Are usually eaten with a spoon
Do not require chewing
Have a smooth texture with no lumps
Hold shape on a spoon
Fall off a spoon in a single spoonful when tilted
Are not sticky
Liquid (like sauces) must not separate from solids
Puréed food must pass two different tests per IDDSI guidelines. These are depicted in the resource material. These tests include:
IDDSI Fork Drip Test: Liquid does not dollop, or drip continuously through the fork prongs . A small amount may flow through and form a tail below the fork.
IDDSI Spoon Tilt Test: Sample holds its shape on the spoon and falls off fairly easily if the spoon is tilted or lightly flicked. Sample should not be firm or sticky.
TIP: I share this system for classifying levels of food and liquid textures as it is increasingly becoming widely used in the U.S.. You may see these levels and terms used by your health care team or on the discharge paperwork you have from the hospital or a treating facility. Please go to their website, IDDSI.org for further detailed information of all the food texture and liquid texture guidelines and tests for each level.
TIP: Additionally, there is no mandate for a healthcare facility to follow or implement any dysphagia classification system. Every facility is different in the terms they use when describing the diet consistencies they provide to their residents/patients. If you or a loved one with dysphagia enter a health care facility and require a special diet consistency for foods and/or liquids, be certain to make the staff aware immediately and that the dietary department has been notified of the modifications needed.
It may be necessary to be vigilant to be certain appropriate departments have been notified and provide the correct diet consistency modifications over the early hours and even days of being admitted into a new setting.
Puréed Food Guidelines in the Home Setting:
It is assumed when a speech-language pathologist gets a referral to see an individual on a puréed diet that they will be receiving food that is smooth and free of lumps. However, not every individual on a puréed diet needs it to be this restricted.
Some individuals can tolerate a pureed food that has a grainy texture to it or tiny bits of food in it. For example, some individuals can tolerate oatmeal, others cannot.
This is where the need for a speech pathologist comes in. They will assess the etiology or root cause of the swallowing problem and work with the individual and/or caregivers to trial levels that are safe and can be tolerated within the confines of a puréed diet.
A speech pathologist will provide education and teaching on dysphagia. Teaching may cover compensatory safe swallowing strategies that may be effective, positioning or aids that may facilitate safer swallowing, and when or if re-evaluations are appropriate.
A speech pathologist can assist in teaching how to modify textures of various foods into a purée. This will help you prepare a greater variety of foods a person is eating for improved compliance of the diet consistency and health of the individual.
Conclusion:
Guidelines and the tests recommended by IDDSI help an individual and/or caregiver feel confident and comfortable in preparing puréed foods correctly. If you are struggling with what foods to purée and how to purée them talk with your primary care physician about a referral to work with a speech pathologist.
Are you concerned that your loved one is having swallowing difficulties but don’t know for sure? What signs should you be looking for that would indicate red flags for a swallow problem?
You are not alone as swallowing problems are common in older people. Swallowing may seem like a simple task, buts it’s actually a complex process involving many muscles and nerves working together in a timely fashion to be normal. When something disrupts this process, it can lead to various swallowing problems , medically known as dysphagia.
It can be very overwhelming to navigate this aspect of caregiving. As a speech pathologist I have worked with numerous individuals and their families and caregivers facing swallowing challenges. I’d like to share some important information to help you recognize the red flags that may indicate a swallowing problem in your loved one.
In this blog post, we’ll explore common signs and symptoms of swallowing problems from a caregiver’s perspective. I will give you the information you need to know and what steps to take next. By knowing what to watch for and what to report to your medical providers, you are playing a crucial role in identifying a swallowing problem.
The four phases of swallowing:
On my first visit to see an individual, I may have information in their chart about a known swallowing problem and the etiology or cause for the dysphagia diagnosis. Other times, I am going in blind with no information other than a speech order for a swallowing evaluation.
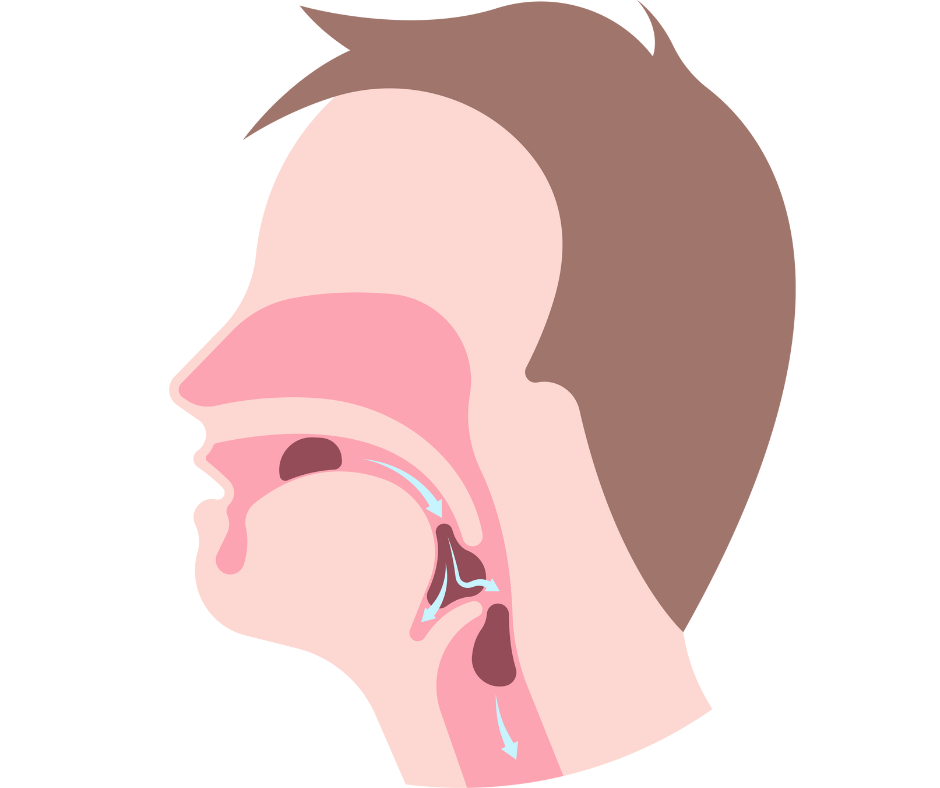
The act of swallowing is segmented into four phases: oral preparatory phase, oral phase, pharyngeal phase and esophageal phase. Depending on what and where you read, these phases can be named differently and can be broken down into different number of phases. There can be a disorder or problem in one phase only of the swallow or a combination of problems in two or more parts of the swallow.
Swallowing problems can be of a sudden onset nature, but more commonly they have existed over several weeks, months or even years. Over time, individuals with swallowing difficulties adapt their eating habits or modify their diets by avoiding foods that trigger symptoms or have learned a strategy to help them swallow.
These adaptations may help them cope with their problem, but it does not address the underlying issue. This lack of awareness, fear or embarrassment, denial or adaptations without addressing the issue could lead to or exacerbate poor nutrition, weight loss issues, risk of dehydration, risk of respiratory infections and overall contribute negatively to health and wellbeing.
Let’s look at each phase of swallowing , identify signs of common swallow problems and potential causes for each problem. These phases are dynamic and overlap. By no means is this a complete and exhaustive list. Identifying signs is recognizing a potential problem, but is not indicative of a swallow problem.
COMMON SIGNS AND SYMPTOMS OF DYSPHAGIA:
PHASES OF SWALLOW
SIGNS OF SWALLOW PROBLEM
POTENTIAL CAUSE OF PROBLEM
1. ORAL PREPATORY PHASE
DROOLING, LOSS OF FOOD OR LIQUID FROM LIPS
LIP CLOSURE: LIPS AREN’T CLOSING AROUND CUP, STRAW OR UTENSIL; DECREASED LIP STRENGTH; DECREASED LIP RANGE OF MOTION; DECREASED AWARENESS (COGNITION); DECREASED SENSATION (PARALYSIS); EXCESS SALIVA WITH POOR ABILITY TO MANAGE
FOOD SCATTERED THROUGHOUT MOUTH VS STAYING TOGETHER IN A FORMED BOLUS
TONGUE MOVEMENT: TONGUE IS NOT MANIPULATING FOOD OR LIQUID IN THE MOUTH; TONGUE IS NOT SHAPING FOOD ; TONGUE IS NOT MOVING FOOD TO TEETH FOR CHEWING; DECREASED TONGUE STRENGTH AND RANGE OF MOTION; DECREASED AWARENESS (COGNITION); DECREASED SENSATION (TONGUE RESECTION, RADIATION OR NERVE DAMAGE, PARALYSIS)
MINIMAL OR NO CHEWING ; MASHING FOOD AGAINST ROOF OF MOUTH VS CHEWING;
CHEWING/MASTICATION: NO TEETH; LACKING TEETH; POOR DENTITION; PAIN WITH CHEWING; MOUTH SORES; CAVITIES/INFECTIONS; ILL FITTING DENTURES; LACKS ROTARY CHEWING; HOLDS FOOD IN MOUTH VS CHEWING (COGNITION); PROBLEMS WITH JAW OPEN AND CLOSING; DRY MOUTH; LACKS SALIVA TO MIX WITH FOOD
FOOD POCKETING OR GETTING STUCK IN CHEEKS
PARALYSIS SIDE OF FACE; CHEEKS LACK MUSCLE STRENGTH AND TONE TO KEEP FOOD OUT OF CHEEK ; LACKS AWARENESS (COGNITIVE); DECREASED TONGUE MOVEMENT TO CLEAR FOOD FROM CHEEK
EXCESSIVE CHEWING; TAKES A LONG TIME TO EAT; HOLDING FOOD IN MOUTH
FOOD TEXTURE TOO CHALLENGING ; FATIGUE; SWALLOW GETS WORSE AS MEAL PROGRESSES; COGNITIVE PROBLEM; DECREASED AWARENESS -FORGETTING TO SWALLOW; LACK RECOGNITION OF FOOD; INATTENTION
2. ORAL PHASE
FOOD REMAINING IN MOUTH AFTER SWALLOW
TONGUE ELEVATION: TONGUE IS NOT ELEVATING TO ROOF OF MOUTH, TONGUE IS NOT PUSHING FOOD OR LIQUID UPWARD AND BACKWARD TOWARD BACK OF MOUTH; REDUCED TONGUE MOVEMENT; REDUCED TONGUE STRENGTH; TONGUE NOT ABLE TO PROPEL BOLUS BACKWARDS; TONGUE NOT RETRACTING FAR ENOUGH TOWARDS BACK OF MOUTH
COUGHING OR CHOKING BEFORE THE SWALLOW
TONGUE IS NOT MANAGING FOOD OR LIQUID TO KEEP TOGETHER AND IT IS PREMATURELY GOING DOWN THROAT BEFORE SWALLOW IS TRIGGERED; REDUCED TONGUE STRENGTH
HOLDING FOOD IN MOUTH AND WAITING FOR A SWALLOW
TIMELY SWALLOW: UNABLE TO TRIGGER A SWALLOW OR DELAY IN SWALLOWING; TONGUE WEAKNESS AND NOT PUSHING FOOD TO BACK OF MOUTH
3. PHARYNGEAL PHASE
FOOD OR DRINK GOING UP NOSE OR COMING OUT NOSE
SOFT PALATE ELEVATION: THE SOFT PALATE IS NOT ELEVATING TO CLOSE OFF NASAL PASSAGE TO PREVENT FOOD OR LIQUID FROM ENTERING NASAL CAVITY DURING THE SWALLOW
COUGHING OR CHOKING DURING OR AFTER THE SWALLOW
FOOD OR LIQUID PENETRATING INTO THE LARYNX; DECREASED AIRWAY PROTECTION; ASPIRATION -FOOD AND/OR LIQUID GOING INTO THE LUNGS; DECREASED LARYNGEAL ELEVATION; POOR TIMING OR UNCOORDINATED TIMING OF MUSCLES; VOCAL CORD PROBLEMS
FEELING OF FOOD CAUGHT IN THROAT; THROAT CLEARING; COUGHING
PHARYNGEAL CONSTRICTION: DECREASED PHARYNGEAL CONSTRICTION; FOOD RESIDUAL IN THROAT AFTER THE SWALLOW; FOOD OR LIQUID REMAINING ON THE WALLS OR IN POCKETS OF THE THROAT AFTER THE SWALLOW
4. ESOPHAGEAL PHASE
FEELING OF FOOD CAUGHT IN THROAT – AT TOP OF ESOPHAGUS
UPPER ESOPHAGEAL SPHINCTER: SPHINCTER NOT OPENING TIMELY OR WIDE ENOUGH FOR FOOD OR LIQUID TO PASS FROM THROAT INTO THE ESOPHAGUS; HAS TO SPIT FOOD BACK OUT; GAGGING, CHOKING AND COUGHING
BURPING, PAIN, DISCOMFORT IN THE CHEST;BURNING IN THE CHEST; DISCOMFORT UPPER ABDOMEN
HEARTBURN OR ACID REFLUX
BITTER TASTE , BURPING UP UNDIGESTED FOOD, A FEELING OF THROWING UP ; FEELING FOOD MOVING UP AND DOWN IN YOUR CHEST
REGURGITATION: SYMPTOMS OF GERD /REFLUX
FEELING OF FOOD AND/OR PILLS, GETTING STUCK IN CHEST; FEELING OF FULLNESS IN ESOPHAGUS
POTENTIAL ESOPHAGEAL ISSUES ; NARROWING OF ESOPHAGUS; DECREASED TIMELY EMPTYING OF THE ESOPHAGUS; HERNIA; STRICTURE; WEBBING ETC,.
COGNITION & DYSPHAGIA:
There is no medical term called cognitive dysphagia but cognition plays a crucial role in the swallowing process. Cognitive dysphagia could be used to describe dysphagia that is primarily driven by cognitive impairments such as dementia and traumatic brain injuries. The etiology of the swallowing problem is cognitive vs. structural or a neuromuscular problem.
Cognitive factors can certainly contribute to swallowing difficulties in some individuals. Cognitively impaired persons may have impairments in the areas of attention, memory, problem solving abilities, and sensory perception, all of which play a role in the swallowing process. It is important that cognitive functioning is taken into consideration when assessing a person for dysphagia and when developing a treatment plan.
EMOTIONAL TOLL OF DYSPHAGIA:
The most obvious signs and symptoms of a swallowing problem are physical in nature. However, dysphagia can have a significant impact on an individuals emotional toll and social habits. Below are additional red flags to observe for or questions to ask your loved ones when considering if your loved one may have a swallowing problem:
Eating or drinking or taking medications is stressful
One does not want to eat in public places or outside of the home
One does not find enjoyment or pleasure in eating any longer
Your loved one is not able to eat the foods they enjoy
Ones social life has changed because of their swallowing problem
Swallowing problem is causing stress, anxiety and/or depression
Not eating, drinking or taking medications because of swallowing problem
Fear of choking , fear of not being able to breath or maybe even die
NEXT STEPS TO TAKE:
If your loved one or someone you are caregiving for is experiencing swallowing difficulties, it is crucial for them to seek an assessment from medical professionals. Here are suggested steps to take:
Schedule An Appointment with Their Primary Care Physician: Your PCP can conduct an initial assessment , discuss the symptoms, and determine the appropriate plan of care.
Be Prepared to Describe Symptoms: Hopefully the most common red flags listed above will give you the knowledge to talk about the physical and/or emotional characteristics of your particular swallowing problem. It may be helpful to write these down ahead of your appointment so to be thorough and exact in describing what your loved one is experiencing.
Seek Further Evaluation: Discuss treatment options with your physician. If your physician is in agreement that a diagnosis of dysphagia is suspected, depending on the symptoms a referral to a specialist for further evaluation will be the reasonable next step. This could include a speech-language pathologist, otolaryngologist or ENT (Ear, Nose & Throat doctor), gastroenterologist and/or a neurologist. There are various tests that may be recommended dependent on the type of specialist you see and the type of problem you present with.
Follow Treatment Recommendations: Treatment for dysphagia varies depending on the underlying cause. The healthcare provider will discuss treatment options based on findings from their evaluations. This may include dietary modifications, swallowing exercises, medications, or surgical interventions.
Seek Support: Living with dysphagia can be challenging. Knowledge is powerful in helping you understand and manage your swallowing problems. Speech-language pathologists can provide valuable guidance, information and support. This may include teaching on how to modify textures, , how to position a person for optimal safety for oral intake, compensatory swallowing strategies to reduce risk , teaching on aspiration precautions and reflux precautions, and adaptive utensils, cups and dishes for maximizing independence and oral intake.
Monitor Symptoms: It is vital to follow up with your PCP after a treatment or intervention has been implemented to discuss progress or lack of progress in managing the symptoms of dysphagia. It may be necessary to adjust treatments or seek further diagnostic work ups to get more favorable outcomes.
CONCLUSION:
I am amazed over and over again with how long some individuals live with a swallowing problem and have never mentioned this to their physician before. An appropriate evaluation, diagnosis, and treatment can improve a persons swallowing abilities and improve overall quality of life and health. Swallowing can have a profound impact on daily life. I strongly encourage you seek evaluation and guidance from a qualified healthcare provider for a thorough assessment and dysphagia management plan.